One goal of TKA is to achieve balanced tension within the knee throughout range of motion. This balanced tension is important for implant stability and longevity. A balanced knee has rectangular Flexion and Extension gaps. A balanced knee also has equal sized Flexion and Extension gaps.
The rectangular Flexion and Extension gaps demonstrate that the medial and lateral compartment share equal tension. The angle of bone cuts and the surrounding soft tissue tension can both affect the balance of the flexion gap (90°) and extension gap (0°). Because the gaps are affected by the bone cut and the soft tissue tension, surgeons can adjust either to balance the gaps, and each approach represents a difference school of thought. Some surgeons argue that bone cuts should be used to create rectangular gaps (measured resection), others argue that soft tissue releases should used to create rectangular gaps (gap balancers).
Gap Balancing Technique. In this approach, the soft tissue tension is assumed to be correct (its not altered) and its used to determine bony cuts. The tibial cut is made first and then acts as guide to plan the cuts for the distal femur and posterior femur. Essentially you put a 9 mm block on top of your tibial cut and draw a line across the top of it with the knee in extension. That line that’s where your distal femoral cut will be, and that is your extension gap. Then with the knee in flexion, draw a line across the spacer block and that is where your posterior femoral cut will be, and that is your flexion gap. The tibia cut acts as a foundation to make the femur cuts.
Measured Resection Technique. In this approach, the soft tissue tension is not trusted and will be edited once the bony cuts are made. The bony cuts are made based on anatomic landmarks (or navigation), then a spacer block is used to examine the flexion and extension gaps. If the gaps are not symmetric (trapezoidal) after the bony cuts are made, and assuming the bony cuts were done properly, the imbalance is due to soft tissue changes secondary to a chronic knee deformity. Over time, a varus or valgus deformity will affect the soft tissue tension on the medial and lateral side. If the soft tissue tension becomes unbalanced, it needs to be corrected during surgery. The need for ligament balancing can be evaluated pre-operatively by performing varus-valgus stress x-rays to determine whether the knee deformity is “fixed” or “flexible”. A fixed deformity (does not correct on stress x-ray) will often require ligament balancing.
A stepwise approach for sequential ligament releases, dictated by the type of deformity, is essential to good outcomes.
Posterior ligaments lead to tightness in extension (just bend down and touch your toes, you feel the pull posteriorly in your knee with this hyper-extension stretch). Anterior ligaments lead to tightness in flexion.
Varus deformity.
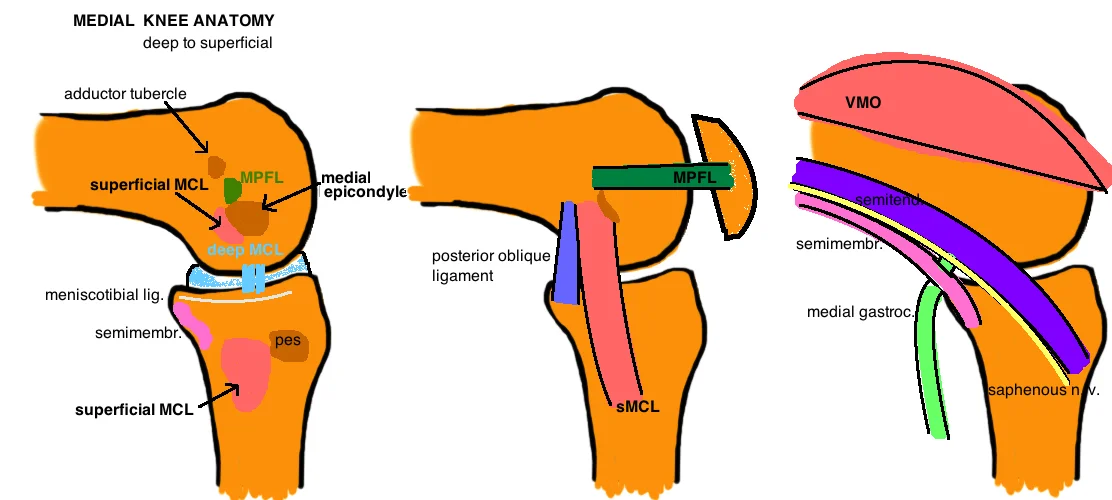
Tight in Flexion. Release the anterior portion of the deep MCL. If still tight anterior release the Pes.
Tight in extension. Release the posterior portion of the deep MCL and capsule. If still tight release some of the superficial MCL. If still tight posterior, release the Semimembranosus. If still tight anterior release the Pes.
Valgus deformity.

Only 10% of knee deformities that require TKA are done for the valgus knee. The Ranawat classification [1] uses 3 grades to describe valgus deformity severity. Grade I is <10° valgus deformity (normal valgus angle is ~ 6°), correctable alignment with stress, and intact MCL and this type accounts for >80% of all valgus knees. Grade II is an angle 10° - 20° degrees, MCL is attenuated but a firm endpoint, and this type accounts for 15% of valgus knees. Grade III is a valgus angle >20° and absent or severely attenuated MCL. This grading scale helps to determine the type of implants and correction that is required.
Soft tissue considerations.
If the MCL is intact, then a primary TKA poly insert can be used. If the MCL is elongated, a constrained poly may be necessary to give sufficient coronal stability. Literature shows there is a risk of recurrent valgus deformity after primary TKA when the MCL is deficient and primary insert is used (even when satisfactory ligament balancing occurs at the time of surgery) [2]. The use of constrained poly effective prevents this recurrence [3]. A constrained insert absorbs more of the joint reactive forces, and the next question is whether stems are necessary to increase the surface area of the bone-implant interface to absorb these greater forces [4]. Some argue that an elongated MCL is still functional and a constrained insert without stems is not at increased risk for loosening. If the MCL is completely absent, a hinge prosthesis should be considered as excessive stress to a constrained insert may cause significant wear and early loosening and post fracture.
MCL attenuation also adds significant challenge to gap balancing. In a varus knee, the tight medial structures are released to match the normal or slight attenuated lateral side (the point is that the lateral side is rarely significantly loose). In the valgus knee however, the MCL can be significantly pathologic, and by releasing the lateral structures to match the enlongated MCL, you can significant increase the size of the gap (because you are using a very pathologic structure as your target), and you may even lengthen the operative leg, require a large poly, and put the peroneal nerve at risk for traction injury.
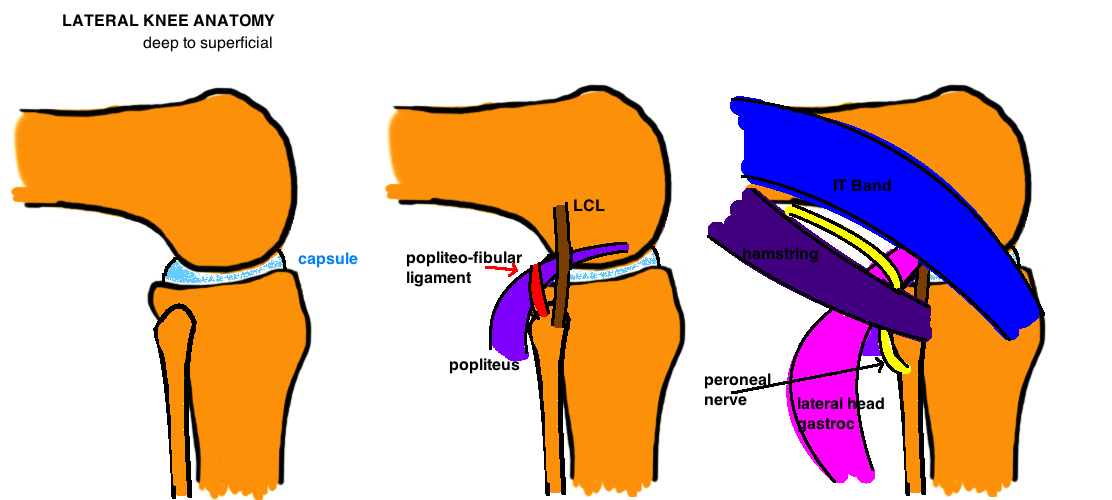
There is debate about the order of soft tissue releases to achieve a balanced gap. Releases should be performed with the knee in extension and the balance should be rechecked after every release. Ranawat recommends “inside-out” technique of pie-crusting the IT band, then the LCL with a no. 15 blade, and making effort to preserve the popliteus. [1] The peroneal nerve is at risk between IT band and Popliteus at the level of the tibial cut. Studies show that LCL release provides the most correction, and some recommend releasing first in cases of severe valgus deformity [5] [2].
Bone considerations.

The valgus knee is uniquely different from the varus knee because bone loss occurs on the lateral femur (in contrast to vaurs knee that shows anterior-medial tibial bone loss. The entire Lateral Femoral Condyle can be significantly hypoplastic (posterior and distal femoral condyles). This is important to identify if the surgeon is measuring femoral rotation by posterior referencing, which typically add 3° to compensate for the difference in sizes between the medial and lateral femoral condyle. In the case of a hypoplastic LFC, the posterior referencing system may need to dial in 5° or more to prevent internal rotation of the femoral component. Additionally, if there is more than 5 mm of deficient bone on the posterior or distal femoral cut, augments should be considered because a cement mantle this large will lead to early loosening. It is important not to chase a large bone defect. If the distal femoral cut does not touch the lateral femur, do not resect additional distal femur because this will raise the joint line, causing patella baja. Similarly, if there is tibial bone loss, measure 4-6 mm off the medial side (non-affected side) to determine the depth of the cut, attempting to cut distal to the defect often removes excessive bone (“apb”: always preserve bone!). The distal femoral cut is often made at only 3° as opposed to the standard 5 – 7° to avoid undercorrection of the deformity.
REFERENCES
1. Ranawat, A.S., et al., Total knee arthroplasty for severe valgus deformity. J Bone Joint Surg Am, 2005. 87 Suppl 1(Pt 2): p. 271-84.
2. Favorito, P.J., W.M. Mihalko, and K.A. Krackow, Total knee arthroplasty in the valgus knee. J Am Acad Orthop Surg, 2002. 10(1): p. 16-24.
3. Easley, M.E., et al., Primary constrained condylar knee arthroplasty for the arthritic valgus knee. Clin Orthop Relat Res, 2000(380): p. 58-64.
4. Anderson, J.A., et al., Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res, 2006. 442: p. 199-203.
5. Krackow, K.A. and W.M. Mihalko, Flexion-extension joint gap changes after lateral structure release for valgus deformity correction in total knee arthroplasty: a cadaveric study. J Arthroplasty, 1999. 14(8): p. 994-1004.