Cigarette smoke contains roughly 70 known carcinogens among over 7,000 chemicals that have the combined effect of decreasing oxygen-carrying capacity of blood, inducing vasoconstriction of peripheral vessels, and leading to tissue hypoxia.
These effects lead to problems with wound healing (nutrients and oxygen isn’t delivered to the surgical site, and impaired collagen synthesis), impaired immunity (lymphocytes aren’t delivered to the site of surgery), and promotion of venous thrombosis. Tobacco likely delays bony ingrowth, and is associated with higher rates of implant loosening.
This leads to more complications and more revision surgery [1] [2].
Tobacco has a negative effect on multiple outcomes. It may increase complication risk up to 50%, and hospital costs were on average $5k higher.
Tobacco cessation programs.
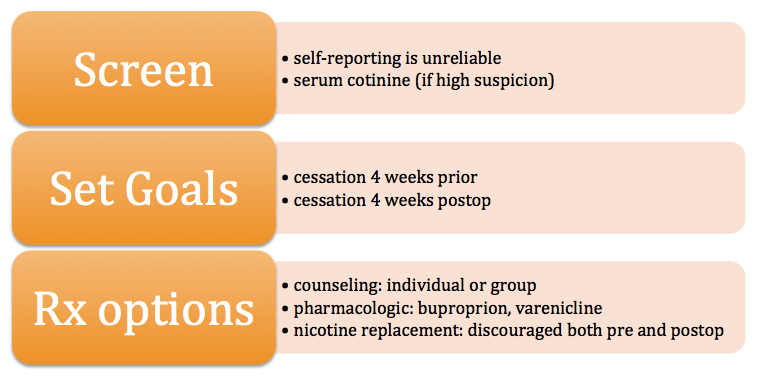
Cessation appears to effectively reduce postoperative complications, particularly SSI, if implemented 4 weeks prior to surgery and maintained 4 weeks following. Benefits of short-term cessation has been supported by multiple other studies in other fields of surgery. Yet current and former smokers retain an increased risk for complication compared to never-smokers [3].
Using a Cessation program encourages about 60% of patients to effectively stop smoking, while only 8% will stop if the extent of intervention is limited to a doctor telling the patient to stop. Overall, paying for a program is less expensive for a hospital than accepting the higher complication rates [4] [5] [6] [7] [8] [9] [10]
Patients can be monitored for smoking through testing for a nicotine metabolite called Cotinine (<10 ng/mL is associated with not smoking), and is detectible for up to 1 week after smoking.
REFERENCES
1. Kapadia, B.H., et al., Tobacco use may be associated with increased revision and complication rates following total hip arthroplasty. J Arthroplasty, 2014. 29(4): p. 777-80.
2. Singh, J.A., et al., Smoking as a risk factor for short-term outcomes following primary total hip and total knee replacement in veterans. Arthritis Care Res (Hoboken), 2011. 63(10): p. 1365-74.
3. Duchman, K.R., et al., The Effect of Smoking on Short-Term Complications Following Total Hip and Knee Arthroplasty. J Bone Joint Surg Am, 2015. 97(13): p. 1049-58.
4. Moller, A.M., J. Kjellberg, and T. Pedersen, [Health economic analysis of smoking cessation prior to surgery--based on a randomised trial]. Ugeskr Laeger, 2006. 168(10): p. 1026-30.
5. Villebro, N.M., et al., Long-term effects of a preoperative smoking cessation programme. Clin Respir J, 2008. 2(3): p. 175-82.
6. Lindstrom, D., et al., Effects of a perioperative smoking cessation intervention on postoperative complications: a randomized trial. Ann Surg, 2008. 248(5): p. 739-45.
7. Moller, A.M., et al., Effect of smoking on early complications after elective orthopaedic surgery. J Bone Joint Surg Br, 2003. 85(2): p. 178-81.
8. Lavernia, C.J., R.J. Sierra, and O. Gomez-Marin, Smoking and joint replacement: resource consumption and short-term outcome. Clin Orthop Relat Res, 1999(367): p. 172-80.
9. Moller, A.M., et al., Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet, 2002. 359(9301): p. 114-7.
10. Thomsen, T., H. Tonnesen, and A.M. Moller, Effect of preoperative smoking cessation interventions on postoperative complications and smoking cessation. Br J Surg, 2009. 96(5): p. 451-61.