Fracture can occur during surgery (intra-op) or after surgery and fractures are treated differently based on this distinction.
INTRAOP FRACTURE
Highest risk is cementless implants with proximal wedge taper design. These design types are made for Dorr C femurs which recognize capacious canal and attempt to fill the large void. However, these wide proximal designs can act as a "log-splitter" in the osteoporotic bone. If a split in the proximal bone (typically around a calcar) occurs while inserting the implant, the implant can be removed, a cable placed around the calcar, and the implant is reinserted, and patients are made full weight-bearing. If the implant however does not feel stable after cabling, a long-stem with diaphyseal ingrowth should be placed. Additionally, a fully coated stem should be used if the fracture occurs distal to the metaphyseal region (this can occur with cylindrical design stems).
LATE FRACTURE
The lifetime risk of a periprosthetic fracture (PPF) is relatively low, the Mayo Registry [1] [2] reported rates of 0.3% in cemented stems and 5.4% in press-fit stems, while other reports suggest about 1% for primary THA and 4% for revision THA. It appears that press fit implants have a higher risk of fracture, although it appears an age-related correlation, whereby patients older than 70 years had a 2.9x risk compared with younger patients, and those over 80 years had a 4.4x risk [3] as compared to cemented stems, which have no age correlation [4].
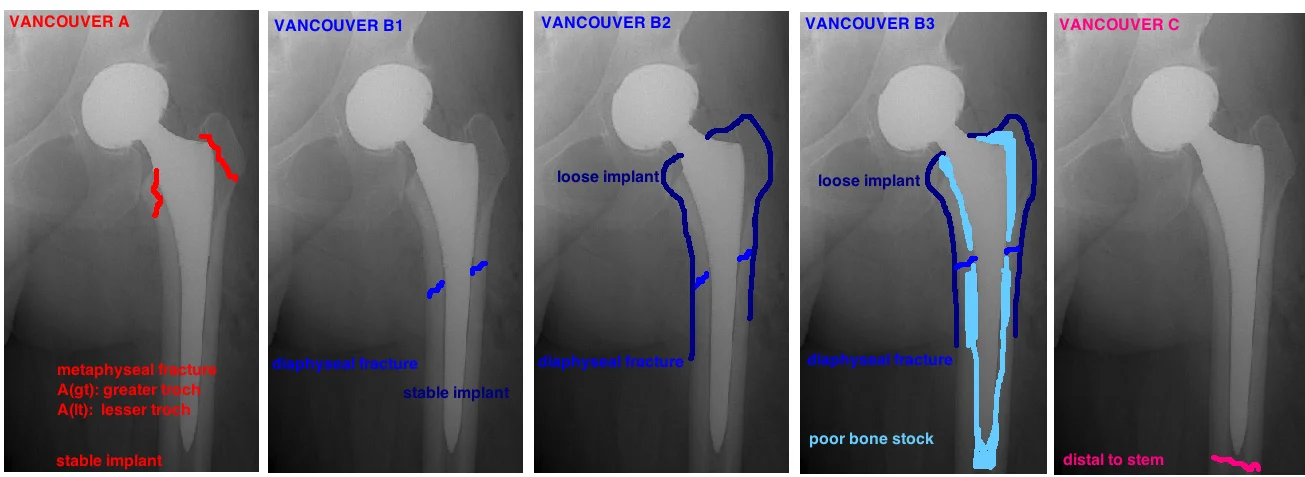
Late fractures are discussed via the Vancouver Classification.
TREATMENT
The key determinants of treatment include: 1) Fracture location, 2) Implant Stability; 3) Bone Stock. These 3 factors are the key points of the Vancouver Classification, which guides treatment decisions [5] [6].
Fracture location. Location falls into three regions. 1) Metaphyseal. 2) diaphyseal around the implant; 3) diaphyseal below the implant. Location is important because it helps determine whether the implant is loose.
Is the Implant Loose? This is the million dollar question. Fractures of the greater troch (Vancouver A) generally do not cause implant loosening. Fractures completely distal to the tip of the stem (Vancouver C) similarly do not cause implant loosening. In such cases, the implant is retain and the fracture is treated as an isolated incident.
In contrast, fractures along the length of the prosthesis (Vancouver B), usually, but not always ,cause implant loosening. The challenge is that its not always easy to identify loosening. And it is critical to identify an implant that is loose because, if its missed, the revision surgery will fail. In fact, studies show higher revision rates for Vancouver B1 fractures (“stable implant”), compared to Vancouver B2 fractures (“loose implant”)…probably because many of the B1 fractures were not truly stable and the implant was subtly loose, and they were misdiagnosed and subsequently failed because they underwent the wrong surgery. Therefore, a fracture around the implant should be considered loose until proven otherwise.
Loosening is evaluated both pre-op and intra-op. Preop evaluation involves looking at the x-rays and comparing them to pre-fracture x-rays for signs of subsidence. Intraop evaluation involves attempting to remove the stem. The general idea is: “If you can knock it loose, then it was loose to begin with”. Also, if the fracture has occurred within 6 weeks of the index procedure, the stem is loose a priori because ingrowth requires at least 6 weeks to occur.
▪ Bone stock. Assessing the bone stock is critical in selecting the proper prosthesis. Periprosthetic fracture most commonly occur in the elderly with significant osteoporosis, or in people with significant osteolysis, which has made the bone thin and highly susceptible to fracture. If the stem is loose and needs revision, it is critical to select the proper implant based on bone stock, because remember that many femoral implants will fail without the proper bone stock [7]. The Vancouver Classification takes bone stock into account, yet the Paprosky Classification is the best guide for correlating bone stock with implant selection. For a full discussion of Femoral Bone Loss, see the section on Osteolysis.
Type A: Fracture occurs in the inter-trochanteric area, usually due to osteolysis. The subclass is based on Greater Troch vs. Lesser Troch. Greater Troch with <2.5cm displacement is protected weight bearing 3 months, if >2.5 cm then it risks nonunion, thus ORIF [8]. Lesser troch fx is rare, little consequence, just treat symptoms [9]
Type B: Fracture occurs around the implant. This risks the stability of the implant, so first assess implant stability. Look for subsidence by comparing height and offset to prior x-rays of the implant.
B1 is a stable implant, and req. ORIF [10]. However, theres shown a higher failure rate with B1 vs. B2 which suggests that many B1 were actually unstable and misdiagnosed, and therefore its critical for the surgeon to fully evaluate the implant during surgery to determine stability, must prove its stable. [11] [12]
B2 is loose implant, req. revision to long-stem that bypasses the fracture by 2 cortical diameters. Its best to place a cerclage calbe at the most proximal aspect of intact distal femur to ensure that there are not hairline fractures that could propagate distally and prevent fixation. Use a tapered fluted stem rather than a cylindrical stem (decreases intraop fractures). Excellent healing rates. [13]

Identification of Vancouver B2 fracture.

Treatment of Vancouver B2 fracture with cables and Wagner-type diaphysial fitting stem
B3 also accounts for the bone stock around the fracture. These are periprosthetic fractures with poor bone stock and loose implant, and thus require long-stem and allograft or a modular prosthesis, and are considerable more challenging to treat.
If there is more than 4-6 cm of scratch-fit in the diaphysis then an extensively porous-coated component can be used, but if there is <4 cm scratch-fit diaphysis, a noncemented tapered fluted stem is needed.
Type C: Fracture occurs distal to stem.
There is no risk to stability of the implant, therefore just perform ORIF, such as using LISS plate, overlap with stem of implant to ensure no stress risers.
OUTCOME
The functional outcome after successful fracture fixation is generally poor [14], with scores worse than THA revision for aseptic loosening [15]. Furthermore, the 1-year mortality rate is about 11% (as compared to 2.9% after elective THA) [16]. Looking at the age-related association with this complication, it appears that older and older patients, with weaker and more osteoporotic bone… are more medically frail, experience this complication. Therefore, the high mortality rate may be less an indication of the injury severity versus an indication of the patients that suffer this complication.
REFERENCES
1. Berry, D.J., Epidemiology: hip and knee. Orthop Clin North Am, 1999. 30(2): p. 183-90.
2. Thomsen, M.N., et al., Fracture load for periprosthetic femoral fractures in cemented versus uncemented hip stems: an experimental in vitro study. Orthopedics, 2008. 31(7): p. 653.
3. Cook, R.E., et al., Risk factors for periprosthetic fractures of the hip: a survivorship analysis. Clin Orthop Relat Res, 2008. 466(7): p. 1652-6.
4. Thien, T.M., et al., Periprosthetic femoral fracture within two years after total hip replacement: analysis of 437,629 operations in the nordic arthroplasty register association database. J Bone Joint Surg Am, 2014. 96(19): p. e167.
5. Masri, B.A., R.M. Meek, and C.P. Duncan, Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res, 2004(420): p. 80-95.
6. Brady, O.H., et al., The reliability and validity of the Vancouver classification of femoral fractures after hip replacement. J Arthroplasty, 2000. 15(1): p. 59-62.
7. Paprosky, W.G., N.V. Greidanus, and J. Antoniou, Minimum 10-year-results of extensively porous-coated stems in revision hip arthroplasty. Clin Orthop Relat Res, 1999(369): p. 230-42.
8. Pritchett, J.W., Fracture of the greater trochanter after hip replacement. Clin Orthop Relat Res, 2001(390): p. 221-6.
9. Pike, J., et al., Principles of treatment for periprosthetic femoral shaft fractures around well-fixed total hip arthroplasty. J Am Acad Orthop Surg, 2009. 17(11): p. 677-88.
10. Parvizi, J. and D.N. Vegari, Periprosthetic proximal femur fractures: current concepts. J Orthop Trauma, 2011. 25 Suppl 2: p. S77-81.
11. Lindahl, H., et al., Risk factors for failure after treatment of a periprosthetic fracture of the femur. J Bone Joint Surg Br, 2006. 88(1): p. 26-30.
12. Lindahl, H., et al., Periprosthetic femoral fractures classification and demographics of 1049 periprosthetic femoral fractures from the Swedish National Hip Arthroplasty Register. J Arthroplasty, 2005. 20(7): p. 857-65.
13. Incavo, S.J., et al., One-stage revision of periprosthetic fractures around loose cemented total hip arthroplasty. Am J Orthop (Belle Mead NJ), 1998. 27(1): p. 35-41.
14. Beals, R.K. and S.S. Tower, Periprosthetic fractures of the femur. An analysis of 93 fractures. Clin Orthop Relat Res, 1996(327): p. 238-46.
15. Young, S.W., C.G. Walker, and R.P. Pitto, Functional outcome of femoral peri prosthetic fracture and revision hip arthroplasty: a matched-pair study from the New Zealand Registry. Acta Orthop, 2008. 79(4): p. 483-8.
16. Bhattacharyya, T., et al., Mortality after periprosthetic fracture of the femur. J Bone Joint Surg Am, 2007. 89(12): p. 2658-62.